The list of cartilage reconstruction procedures mentioned below is not comprehensive, but includes some examples on this field.
Debridement
Debridement is a cleaning procedure in simple words. Debridement doesn't restore damaged cartilage. During this procedure damaged cartilage and loose pieces are removed, which relieves mechanical symptoms such as joint locking, catching and clicking. Torn cartilage flaps are typical reasons for this kind of symptoms. Debridement can be an isolated operative procedure treating minor cartilage lesions, or it can be combined to e.g. meniscus surgery if cartilage flaps are evident. It is relatively inexpensive and easy operative procedure with short postoperative rehabilitation, but it will not produce new cartilage.
Deeper debridement is the first step in cartilage reconstruction procedures. As new cartilage tissue should integrate well not only with the bone, but also with the adjacent cartilage, all non-healthy tissue is removed leaving healthy vertical in relation to bone cartilage borders around damaged area. Calcified cartilage layer is also removed and bone is revealed. It is important also to clean the unhealthy bone with poor blood circulation especially in long-term cartilage defects, where bone reactions is seen.
Deeper debridement is the first step in cartilage reconstruction procedures. As new cartilage tissue should integrate well not only with the bone, but also with the adjacent cartilage, all non-healthy tissue is removed leaving healthy vertical in relation to bone cartilage borders around damaged area. Calcified cartilage layer is also removed and bone is revealed. It is important also to clean the unhealthy bone with poor blood circulation especially in long-term cartilage defects, where bone reactions is seen.
Microfracture
Microfracture belongs to marrow stimulation procedures. It is also relatively low cost one-step procedure more suitable for juveline and adolescent patients with limited size cartilage lesions on weight bearing areas.
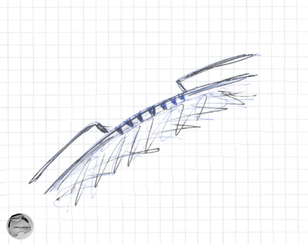
Microfracture includes debridement of damaged cartilage area, and subchondral bone perforation either with owl or by drilling small holes. Multiple holes are made approximately 3-4 mm apart from each other. Bone marrow appears in perforation holes as blood and fat cells forming a blood clot. This blood clot is a base for a new fibrocartilage or mixed hyaline-fibrocartilage formation. This method works better in younger patients. Fibrous tissue doesn't have those properties as a original tissue and is not as durable. That's why microfracture may have a better short-term than a long-term outcome. Rehabilitation after microfracture depends on the addressed area, but usually includes protecting new tissue formation with restriction of weight bearing for 6- weeks and early joint non-weight bearing passive and active mobilisation.
Microfracture includes debridement of damaged cartilage area, and subchondral bone perforation either with owl or by drilling small holes. Multiple holes are made approximately 3-4 mm apart from each other. Bone marrow appears in perforation holes as blood and fat cells forming a blood clot. This blood clot is a base for a new fibrocartilage or mixed hyaline-fibrocartilage formation. This method works better in younger patients. Fibrous tissue doesn't have those properties as a original tissue and is not as durable. That's why microfracture may have a better short-term than a long-term outcome. Rehabilitation after microfracture depends on the addressed area, but usually includes protecting new tissue formation with restriction of weight bearing for 6- weeks and early joint non-weight bearing passive and active mobilisation.
Mosaicplasty
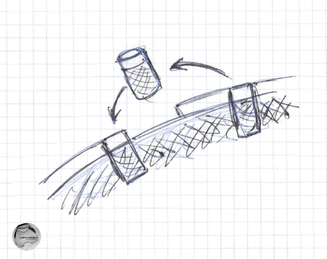
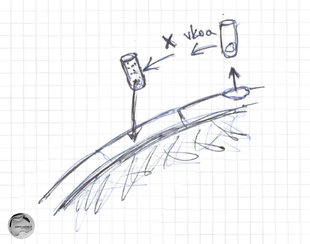
Mosaicplasty is an autogenous osteochondral grafting technique. It includes harvesting cylindrical osteochondral plugs from peripheral femoral area, and transplanting these plugs into a damaged area. Osteochondral grafting aims to provide direct hyaline-like cartilage repair. The depth of osteochondral plugs has to be enough to make it stable, and to shape and cartilage layer thickness has to match the surrounding area. The donor site undergoes natural healing process with fibrocartilage formation. Mosaic-like transplantation of multiple small-sized plugs allows formation of congruent surface and is better for a donor site than harvesting larger grafts.
Mosaicplasty can be performed as an arthroscopic or mini arthrotomy procedure. Post operative rehabilitation includes restriction of weight bearing with progressive return to normal daily activities in 8-10 weeks. High demanding sports activities can be restricted up for 6 months.
Mosaicplasty can be performed as an arthroscopic or mini arthrotomy procedure. Post operative rehabilitation includes restriction of weight bearing with progressive return to normal daily activities in 8-10 weeks. High demanding sports activities can be restricted up for 6 months.
ACI
Articular chondrocyte implantation (ACI) ACI is a cell based treatment option, traditionally performed as a two step procedure. The first procedure is an arthroscopy including biopsy of healthy cartilage from non-weight bearing area of the joint. Chondrocytes are isolated and cultured in laboratory for several weeks. This gives a lot of patients own cartilage cells to be applied on defect area in the second operation. Traditionally it is an open surgery including debridement of damaged area to achieve stable cartilage shoulders and suturing membrane to close this defect area. Cells are injected under this membrane hood to produce new cartilage. If there is also a subchondral lesion, sandwich techniques can be used to fill the defect and seed cultured cell on top of this basement. As in microfracture fibrocartilage or mix hyaline-fibrocartilage is formed. Younger patients tend to have have better outcome after that procedure.
|
|
The content of this website is provided for information only and is not intended to be used for diagnosis or treatment or as a substitute for consultation with your own doctor or a specialist.Email addresses supplied are provided for basic enquiries and should not be used for urgent or emergency requests, treatment of any knee injuries or conditions or to transmit confidential or medical information.
|